Cart
Cart

Vitamin D
01 Nov 2016
Assigned to vitamin D quite passive part in a calcium exchange regulation earlier. Was considered that this vitamin has to be present only at a blood in enough to provide a calcium absorption in an intestine and effective action the Parathyroidin (parathormone, PTG). Now it is known that the vitamin D role in exchange of a calcium is much more active. Though it is called vitamin, actually it represents hormone which together with PTG performs function of the main regulator of concentration of a calcium in a blood. Really, vitamin D possesses typical signs of hormone: 1) it is synthesized in a skin, and in ideal conditions of this synthesis can be quite enough (that is its entering with a nutrition can be and not obligatory), 2) he is had with a blood to other organs where it is activated by strictly adjustable enzymes, 3) its active form (calcitriol) is bound to specific receptors of target tissues that leads eventually to rising of concentration of a calcium in a blood. Besides, today it is known that vitamin D performs also other functions. Calcitriol receptors are available on many cells, including marrow cells, lymphocytes, epidermal cells, cells of islands of a pancreas, muscle and nervous cells; activation of these receptors is followed by the various effects which aren't bound to calcium exchange. Historical information. Vitamin D call two congenerous liposoluble bonds � kholekaltsiferol and ergocalciferol, having ability to prevent or cure of rachitis. Before discovery of this vitamin suffered from a rachitis many children living in the cities of a moderate climatic zone. Some researchers considered that rachitis develops because of shortage of fresh air and sunlight, others saw its reason in features of a delivery. Fair were both points of view as illness managed to be prevented or cured as by addition to a diet of cod-liver oil (from cod liver), and impact of a sunlight (Mellanby, 1919; Huldschinsky, 1919). In 1924 it was shown that the rachitis at animals recovers ultra-violet radiation not only individuals, but also the nutrition consumed by them (Hess and Weinstock, 1924; Steenbock and Black, 1924). These observations led to interpretation of structure of a holekaltsiferol and ergocalciferol. It was established also that these substances gain activity only after a series of biochemical transformations. Processes of activation of vitamin D are studied generally American (DeLuca and Schnoes, 1976) and English (Kodicek, 1974) by researchers.
Chemical properties and sources
Ultra-violet radiation of some sterol of an animal and plant origin turns them into the bonds having activity of vitamin D. The rupture of communication between S-9 and S-10 atoms is for this purpose necessary (though at the same time not all sterola gain antirachitic activity). The main provitamin found in animals is 7-degidrokholesterin which is synthesized in a skin. Under the influence of ultra-violet radiation 7-degidrokholesterin turns in kholekaltsiferol (D3 vitamin)
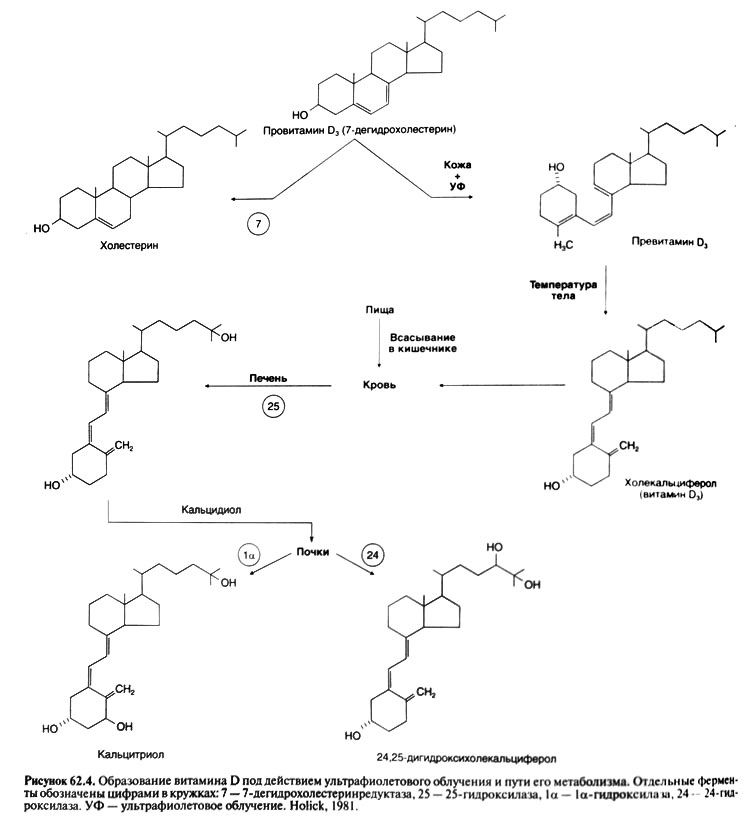
Formation of vitamin D under the influence of ultra-violet radiation and a way of his metapain.
An intermediate photolyte is a provitamin D (a D3 vitamin 6.1-cis-isomer) which collects in a skin at ultra-violet radiation is found (No-lick, 1981). This isomer slowly spontaneously turns into D3 vitamin and sometime after radiation can be its source. The attendee in plants ergosterol represents a provitamin of D (the precursor of D2 vitamin, or an ergocalciferol). Ergosterol and D2 vitamin differ respectively from a 7-degidrokholesterin and D3 vitamin only in existence of double communication between S-22 and S-23 atoms and metilny group at S-24 atom. Vitamin D is a part of many vitamin drugs and is present at the irradiated bread and milk. The substance which is earlier called by vitamin D (it was an admixture of the bonds interfering development of rachitis. At animal some types ability of vitamins D and D3 to prevent rachitis strongly differs, but at the person both of them act almost equally. Further both vitamins we will designate the general term vitamin D
Activation
As the vitamin D arriving with a nutrition, and synthesized in a skin gains biological activity only after a series of transformations. The main active metabolite � calcitriol � is formed as a result of two consecutive hydroxylations of vitamin D. For more details see, for example, in the review of Horst and Reinhardt (1997). Do not forget take Vitamin B12 for better results.
Hydroxylation of vitamin D
It is the first stage of activation of vitamin D as a result of which it is formed caltsidiol. It proceeds in a liver. Reaction is catalyzed by mikrosomalny or mitochondrial 25 hydroxylase in the presence of NADFN and molecular oxygen. Hydroxylation of caltsidiol. From a liver caltsidiol comes to a blood where connects about vitamin - D - svyazy-vayushchim protein (and globulin) plasmas. The final stage of activation of vitamin D � its transformation into calcitriol � occurs mainly in kidneys though such ability also other cells, including macrophages have (Reichel et al., 1989). The hydroxylation of a kaltsidiol is carried out by a 1a-hydroxylase localized in mitochondrions of cells of a proximal canaliculus. NADFN and molecular oxygen participate in reaction. P450 cytochrome, a yellow enzyme and ferredoksin are a part of a 1a-hydroxylase; it represents an oxidase with the admixed functions.
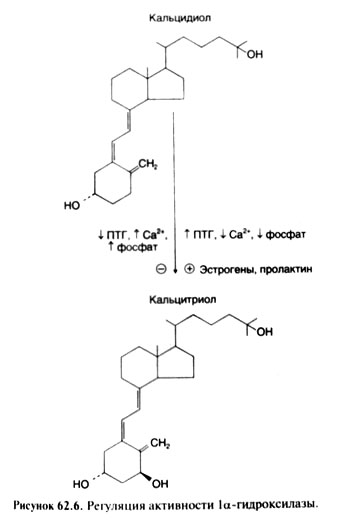
Activity of a 1a-hydroxylase is regulated so that the level of secretion of calcitriol was sufficient for maintenance of normal concentration of a calcium in a blood. At the lowered consumption of vitamin D, calcium and Natrii phosphas activity of enzyme increases, at the increased consumption � decreases. Besides, activity of a la-hydroxylase is enlarged under the influence of PTG, and also probably Prolactinum and estrogens (fig. 62.6). Both a short-term, and long-term regulation of activity of a la-hydroxylase is possible; in the latter case rate of its synthesis changes. Action of PTG is mediated by tsAMF which, apparently, through a series of stages activates the fosfoproteidfosfataza influencing a ferredoksinovy component of a la-hydroxylase (Siegel et al., 1986). According to some data, the hypocalcemia activates a 1a-hydroxylase not only through stimulation of secretion of PTG, but also is immediate. The hypophosphatemia leads to sharp rising of activity of a 1a-hydroxylase (Haussler and McCain, 1977; Fraser, 1980; Rosen and Chesney, 1983). Calcitriol on the mechanism of negative feedback reduces activity of this enzyme, working as it is immediate on kidneys, and through suppression of formation of PTG. Mechanisms of influences of estrogens and Prolactinum on activity of a 1a-hydroxylase aren't known.
Physiology and pharmacology
The main effect of vitamin D is a rising of concentration of a calcium in a blood. Exchange of Natrii phosphas under the influence of vitamin D changes parallel to calcium exchange. At the same time more and more data indicate a role of vitamin D and in many other processes (see below).
Vitamin D maintains normal concentration of a calcium and Natrii phosphas in plasma by means of the following mechanisms: 1) intensifying of an absorption of these ions in a small bowel, 2) their release from bones, 3) depression of their renal egestion. It is difficult to estimate an immediate role of vitamin D at mineralizations of a bone tissue. Was considered that it provides only concentration of a calcium and Natrii phosphas, sufficient for bone formation, in plasma. However now it is known that vitamin D renders both indirect, and direct influence on the cells participating in updating of a bone tissue.
The mechanism of effect of calcitriol is similar to that of steroid and thyroid hormones. Calcitriol is bound to intracellular receptors of cells targets, and hormone - a receptor complex interacts with DNA, changing a transcription of genes. Kaltsitriolovy receptors belong besides to superfamily, as receptors of steroid and thyroid hormones (Evans, 1988; Pike, 1992). Calcitriol causes also bystry (apparently, extra genomic) effects (Barsonyand Marx, 1988).
Calcium absorption in an intestine. Disturbance of an absorption of a calcium in an intestine at rats with deficiency of vitamin D is revealed more than 50 years ago. Introduction by such animal of an active form of vitamin already in 2 � 4 h accelerates movement of a calcium from an intestine, mucous to a serous cover. Mechanisms of this effect aren't absolutely clear (Wasserman, 1997). Relatively induction of one protein from family small calcium binding proteins (calbindin) is early observed. Some researchers consider what calbindin promotes transfer of a calcium through a brush border and its diffusions to a basolateral membrane of enterocytes. Others, noting disharmony of level of calbindin to calcium transport (Nemere and Norman, 1986,1988), believe that calcitriol stimulates endocytosis by means of which a calcium from a lumen of an intestine gets to vesicles of cells of enterocytes. These vesicles merge with lysosomes which deliver a calcium to basolateral membrane from where it also comes to a blood (Cancela et al., 1988). Mechanisms by means of which calcitriol strengthens such transport of a calcium aren't known. Release of calcium from intestine cells in a blood is carried out by calcium pumps of a cellular membrane which number under the influence of calcitriol is enlarged (Wasserman, 1997). Terms of development of effects of calcitriol in animals with an avitaminosis of D testify to the genomic mechanism of its action, however for lack of an avitaminosis calcitriol, working probably through membranous receptors, is also capable to cause fast (within minutes) rising of transport of a calcium (Cancela et al., 1988). Mobilization of a calcium from bones. Though at animals with vitamin deficiency D content of mineral substance in bones is obviously reduced, ability of this vitamin to directly stimulate a mineralization remains unproven. It is considered that vitamin D provides a normal mineralization of bones only by maintenance of concentration of a calcium and Natrii phosphas in a blood due to intensifying of an absorption of these substances in an intestine (Stem, 1980). Really, vitamin - a D-dependent rachitis like II at children is successfully treated i.v. by administration of calcium and Natrii phosphas (see below). On the contrary, physiological doses of vitamin D strengthen washing away of a calcium from bones, and high doses sharply accelerate updating of a bone tissue. Though at animals with remote parathyroid glands influence of calcitriol on resorption of a bone tissue is weakened, correction of a hyperphosphatemia restores this influence (Stem, 1980). Thus, PTG and calcitriol strengthen a resorption of a bone tissue independently from each other.
Mechanisms of the stimulating influence of caltsitriol on updating of a bone tissue are studied only partially. It is established that many interconnected factors (Haussler, participate 1986 in this influence; Reichel et al., 1989). Mature osteoclasts, apparently, are deprived the caltsium receptors and aren't sensitive to caltsitriol, however caltsitriol stimulates movement of cages predecessors to the resorption centers, as well as acquisition with these cages of functions of mature osteoklast (Mimuraet al., 1994). Sharp violation of this reaction on caltsitriol, and also on other substances stimulating a resorption is characteristic of osteopetrosis (at whom the resorption of bone tissue is slowed down). Calcium receptors are available in osteoblasts, and caltsitriol stimulates development with these cages of a number of proteins, including osteocaltsin (Vit - the min.-to-dependent protein containing the remains at-carboksiglu-tamin acid) and SILT-1 (tsitokin, strengthening a resorption of a bone tissue) (Spear et al., 1988).
Renal egestion of calcium and Natrii phosphas
Vitamin D independently reduces an egestion of calcium and Natrii phosphas. Probably, it strengthens their reabsorption in a proximal canaliculus. Value of this effect of vitamin D remains obscure.
Other effects
Now it is established that calcitriol influences not only calcium exchange. Calcitron receptors are present at many cells (Pike, 1992). Under the influence of calcitriol maturing and a differentiation of lymphocytes and monocytes accelerate, and also production of cytokines raises (more detailed about influence of calcitriol on immune system see in the review of Amento, 1987). Particular interest is attracted by ability of calcitriol to oppress a proliferation and to cause a differentiation of tumor cells (van Leeuven and Pols, 1997). Search of analogs of calcitriol which, keeping this action on cells, don't cause rising of concentration of a calcium in plasma is begun. Such substances could be used as antitumoral agents. As calcitriol oppresses a proliferation of keratinotsit and accelerates their differentiation, perhaps, it will find application in treatment of a psoriasis (Kragballe, 1997).
Deficiency of vitamin D at advanced age more than doubles risk of development of senile dementia and Alzheimer's disease, the international group of researchers whose work is published in the Neurology magazine found out.
Dependence between the content of vitamin D in a blood and the volume of fatty tissue are proved. The more you vitamin D, the have less fat and the more muscle bulk. Laboratory researches showed that muscle cells make less Myostatinum under the influence of vitamin D. Also it was revealed that muscle cells with deficiency of vitamin D split muscular tissue quicker.
Scientists at Stanford University conducted the researches on animals devoted to vitamin D - to calcitriol during which its anti-estrogenic effect was studied. The results published in the Endokrinologiya magazine say that calcitriol influences generally fatty tissue that can be interesting to bodybuilders. Besides, it strengthens effects of such anti-estrogens as ����������, letrozole and ����������. If it is possible to transfer results of researches on mice to people that turns out that in human cells production of Oestradiolum will decrease in process of augmentation of concentration of calcitriol in an organism. This fact can be interesting to bodybuilders as the smaller quantity of Oestradiolum means retardation of body height of fatty cells, and also decrease of their sizes. Besides, depression of emergence of a gynecomastia. The experiment showed that reception of vitamin D strengthens effect of an arimideks, ekzemestan and letrozole. As representatives of the western civilization, as a rule, have too low concentration of vitamin D in a blood, it is possible to assume that the athletes using AAS can gain additional effects of aromatase inhibitors if combine it with reception of the additives containing this vitamin.
Absorption, metabolism and elimination
Vitamin D is usually prescribed inside, and in most cases it is well soaked up. Both D2 vitamin, and D3 vitamin are soaked up in a small bowel, but comprehensibility of the last it is probable, above. In what department of a small bowel the greatest number of vitamin D is soaked up, depends by nature foodstuff. The main part of the soaked-up vitamin D is found as a part of chylomicrons in a lymph in the beginning.
An important role in the course of an absorption of vitamin D is played by the bile which is especially present at it desoxycholeic acid. Therefore at lesions of a liver or cholic ways the absorption of vitamin D is significantly broken.
The soaked-up vitamin D connects with arglobuliny plasmas � vitamin - About - the binding protein. Vitamin B to plasma makes 19 � 25 h, but in fatty tissue - is much longer.
As already it became perceptible, in a liver vitamin D turns in caltsidiol which also connects about vitamin - About - the binding protein. Caltsidiol has larger affinity to this protein, than initial bond. Caltsidiol is the main form of vitamin D in a blood; its T1/2 � 19 days. At the person concentration of a caltsidiol is normal peer plasma to 15 � 50 ng/ml though rising of the PTG level and acceleration of updating of a bone tissue can arise already at concentration lower than 25 ng/ml. Calcitriol T1/2 is peer plasma of the person to 3-5 days; 40% of the entered dose are removed for 10 days (Mawer et al., 1976). The renal 24 hydroxylase turns calcitriol (1,25-digidroksikhapekaltsiferol) in 1,24,25-trigidrok-sikholekaltsiferol, and caltsidiol (25-gidroksikholeka-ltsiferol) � in 24,25-digidroksikholekaltsiferol. This enzyme is induced by calcitriol and inhibited by the factors stimulating a 1a-hydroxylase. As 1,24,25-trigidroksikholekaltsiferol, and 24,25-di-gidroksikholekaltsiferol have smaller activity, than calcitriol, and probably represent the excreted metabolites. The metabolism of calcitriol is carried out also by oxidation of a side chain.
Vitamin D is removed generally with bile, in urine only a small part of the entered vitamin is found. Vitamin D and its metabolites are exposed to an active enterohepatic circuit therefore at the patients with an intestinal anastomosis who are suffering from an inflammation of a small bowel or transferred a resection of its larger sites, disturbance of an absorption of vitamin leads to vitamins deficiency.
Serious consequences of interaction of vitamin D with Phenytoinum and Fenobarbitalum are described. At patients, it is long receiving anticonvulsants, the rachitis and osteomalacy were sometimes observed. However these drugs are more often, reducing a calcium absorption in an intestine, promote development of an osteoporosis with fast updating of a bone tissue (Weinstein et al., 1984). At the patients accepting such agents, concentration of caltsidiol in plasma is reduced therefore it was supposed that Phenytoinum and Fenobarbitalum accelerate transformation of vitamin D into inactive metabolites (Hahn et al., 1972). However at most of the patients receiving anticonvulsants, concentration of calcitriol in plasma remains normal (Jubiz et al., 1977). These drugs accelerate also hepatic metabolism of vitamin K and slow down synthesis of vitamin-to-dependent proteins, for example an osteokaltsin.
Requirements and units of measure
The exhaustive report of data on the preventive needs for vitamin D was made by Committee on a delivery of the American academy of pediatrics (Committee on Nutrition, 1963). Since 1919 when Mellanbi established a possibility of prevention of rachitis by means of cod-liver oil (from cod liver), there passed many years. Now this disease meets in the USA very seldom. If in tropical countries prophylaxis of rachitis is provided by solar radiation, then in the countries with a temperate climate, especially in the winter, insolation of a skin is insignificant why there is a need in additional reception of vitamin D.
Earlier special nutritional supplements were necessary for satisfaction of daily needs for vitamin D. Now enrich with this vitamin foodstuff (especially dairy products, products from shredded grain and candy) therefore at any age there is a danger of its excess consumption. Need for additional reception of vitamin D depends not only on age or a condition of an organism (for example, pregnancy or lactemia), but also on structure of a nutrition. Excess consumption of vitamin can lead to serious consequences; at children only 1800 ME vitamins D (see below) can slow down body height. Therefore it is necessary to recommend additional reception of vitamin only after careful studying of a diet.
Irrespective of vitamin D sources its consumption in a dose of 400 ME/days completely provides prophylaxis of rachitis and normal body height of newborns (including prematurely born). This quantity is probably enough for people of any age, including teenagers. Some data indicate ascending of need for vitamin D at pregnancy and lactemia, but 400 ME/days have to be enough also at these states.
The international unit (ME) is equivalent to biological activity of 0,025 mkg of holekaltsiferol (that is 1 mg of holekal-tsiferol supports 40 000 ME).
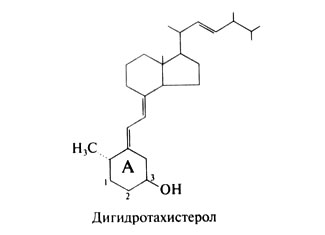
Earlier biological activity of vitamin D and its derivatives was determined by ability to prevent rachitis. Such method is still used in the experimental purposes. Vitamin D derivatives. Appreciable interest is attracted by a possibility of use of a series of derivatives of vitamin D in an experiment and clinic. One of them � Dihydrotachysterolum � represents the restored D2 vitamin. Its structural formula following;
On antirachitic activity Dihydrotachysterolum is about 450 times more weak than vitamin D, but stimulates mobilization of a calcium from bones in high doses much stronger, than vitamin D. For this reason Dihydrotachysterolum is applied to maintenance of normal concentration of a calcium in a blood at hypoparathyrosis.
Dihydrotachysterolum is hydroxylated with education 25 hydroxydihydrotachysterolums which, apparently, and affects an intestine and bones. This substance works and at rats with remote kidneys � means, its activity doesn't depend from 1-hydro-ksilirovaniya in kidneys and consequently, and from the factors operating on a 1a-hydroxylase. In Dihydrotachysterolum molecule the ring And is developed in such a way that the hydroxylic group at S-3 atom holds approximately the same spatial position, as hydroxylic group at S-1 atom in calcitriol molecule. For this reason probably 25-hydroxydihydrothat-histerol without additional hydroxylation it is capable to be bound to kaltsitriolovy receptors.
Synthetic derivative D3 vitamin � alfacaltsidol (1a-gidroksikholekaltsiferol) � contains hydroxylic group in 1a-situation. Mikrosomalny enzymes of a liver easily hydroxylate S-25 atom, turning alfacaltsidol into calcitriol. In experiences on chickens drug so activly stimulates a calcium absorption in an intestine and a mineralization of bones, as calcitriol. As alfacaltsidol doesn't need a hydroxylation in kidneys, it can be applied at a renal osteodystrophy. The USA uses this drug only in experiments.
Synthetic derivative D3 vitamin � alfacaltsidol (1a-gidroksikholekaltsiferol) � contains hydroxylic group in 1a-situation. Mikrosomalny enzymes of a liver easily hydroxylate S-25 atom, turning alfacaltsidol into calcitriol. In experiences on chickens drug so activly stimulates a calcium absorption in an intestine and a mineralization of bones, as calcitriol. As alfacaltsidol doesn't need a hydroxylation in kidneys, it can be applied at a renal osteodystrophy. The USA uses this drug only in experiments.
Content of vitamin D in some foodstuff
Product - Content of vitamin D, mkg/100 of a product
Liver of mackerel - 1500
Liver of flounder - 50-100
Cod liver - 1.5
Herring - 0.37-2.5
Cod - 0.125
Mackerel - 0.125-0.175
Beef liver - 0.025
Egg (yolk) - 0.013-0.05
Summer butter - 0.025
Winter butter - 0.008
Calcitriol analogs
Calcipotriol contains double communication between S-22 and S-23 atoms, hydroxylic group (in a S-configuration) at S-24 atom, and S-25, S-26 and S-27 atoms form a cyclopropane ring. This bond has the same affinity to receptors, as calcitriol, but its activity as calcium exchanger makes only 1% of activity calcitriol! The possibility of use of calcipotriol at a psoriasis was widely studied (hl. 65), for this purpose ointment is already produced. Clinical tests showed that calcipotriol � effective and safe local remedy for a psoriasis, even a little more effective, than glucocorticoids. The mechanism of action of calcipotriol at a psoriasis remains to unknown.
Parikaltsitol � synthetic derivative calcitriol which suppresses formation of PTG, but in a therapeutic dose doesn't cause hypercalcemia. In the USA this drug is allowed for use at a secondary hyperparathyreosis for patients with HPN.
The potent inhibitor of an expression of a gene of PTG which is only poorly influencing an intestine and a bone tissue appeared 22-Oaxaca-ltsitriol. Therefore it is expedient to use it at excess formation of PTG at patients with HPN or even with primary hyperparathyreosis (Finch et al., 1993).
Vitamins deficiency and hypervitaminosis
Vitamin D deficiency. Under vitamin D deficiency the absorption of calcium and Natrii phosphas is broken. As a result concentration of calcium in blood decreases; it stimulates secretion of PTG which causes mobilization of a calcium from bone tissue. Concentration of Natrii phosphas in plasma remains lowered as rising of the PTG level in blood strengthens Natrii phosphas egestion with urine. For children this leads to an insufficient mineralization of the formed osteal and cartilaginous matrix and to development of rachitis. Bones of the patient remain soft and under gravity of a body in a characteristic way are deformed.
For adults vitamin D deficiency leads to osteomalacy at which not mineralized organic matrix collects in bones. The expressed osteomalacy can be followed by severe pains and hypersensibility of bones. Also muscular delicacy, especially large proximal muscles is usually observed. The reason of osteomalacy isn't absolutely clear; perhaps, the disease is bound to hypophosphatemia and lack of influence of vitamin D on muscles. Sharp deformations of bones arise only at late stages.
Low concentration of caltsidiol in blood (less than 8 ng/ml) is a reliable diagnostic sign of osteomalacy.
Hypervitaminosis of vitamin D. Short-term or long reception of large amounts of vitamin D or hypersensibility can lead to disturbances of exchange of calcium with the corresponding symptomatology. Effect of vitamin D depends on its entering from the outside, rates of its synthesis in an organism and sensitivity to it tissues. For some babies the increased reaction already for small doses of vitamin D becomes perceptible. For adults excess administration of drugs of vitamin D can be the cause of a hypervitaminosis of vitamin D or excess consumption by supporters of amateur diets. Sometimes the hypervitaminosis of vitamin D at children arises owing to casual reception of an adult dose.
The amount of vitamin D causing hypervitaminosis at different people variously. By rough estimates, at the person with normal function of parathyroid glands and normal sensitivity to vitamin D the hypervitaminosis can develop at long consumption of vitamin D in number of 50 LLC ME/sut and more. Hypervitaminosis of vitamin D is especially dangerous to the persons accepting cardiac glycosides as the hypercalcemia strengthens toxic effect of these drugs (hl. 34 and 35).
Clinical picture. The first implications of hypervitaminosis of vitamin D are bound to a gaperkalydiyemiya (see above). Also gaperkalydiyemiya at hypervitaminosis of vitamin D, as a rule, is caused by very high level of caltsidiol in blood whereas concentration of PTG and calcitriol usually (though not always) are reduced.
Children have only one episode of hypercalcemia, even medium-weight, can lead to a full stunt for 6 months and more, and lag in body height sometimes remains for the rest of life.
Toxic effect of vitamin D can be shown also at a fetus. There is a dependence between excess consumption of vitamin D by mother (or sharply increased her sensitivity to vitamin) and not heriditary nadklapanny stenosis of an aorta at fetus. For children this defect often is followed by other symptoms of hypercalcemia. Hypercalcemia of mothers can lead also to the oppression of function of parathyroid glands at newborns which is shown hypocalcemia, tetany and epileptic seizures.
Treatment. It is necessary to stop immediately reception of vitamin D and to pass to a diet with the low content of calcium. Prescribe glucocorticoids and plentiful drink. These measures lead to normalization of level of a calcium in a blood, to depression of its contents in soft tissues and to significant improvement of function of kidneys (if only their lesion didn't go too far).
Use
On sale there are many drugs of vitamin D. Ergocalciferol represents pure D2 vitamin; it is prescribed inside, in oil and i.v. Dihydrotachysterolum is the crystalline substance received by D2 vitamin restoration. Dihydrotachysterolum and a caltsife-diol (25-gidroksikholekaltsiferol) prescribe inside. Calcitriol (1,25-digidroksikholekaltsiferol) is prescribed both inside, and i.v.
Indications to use of vitamin D can be divided into four groups: 1) prophylaxis and treatment vitamin - a D-scarce rachitis, 2) treatment of other types of rachitis and renal osteodystrophy, 3) treatment of a hypoparathyrosis, 4) prophylaxis and treatment of an osteoporosis.
Vitamin - D-scarce rachitis
As the reason of this state serves the insufficient insolation or deficiency of vitamin D in a nutrition In the USA and other countries where foodstuff is enriched with vitamin D, it meets extremely seldom. The children receiving enough the foodstuff enriched with vitamin D don't need its additional reception. However when feeding by women's milk or nonenriched nutritious admixtures children need to prescribe in addition vitamin D according to 400 M E / days. Usually recommend to accept vitamin D together with vitamin A. There is a number of the drugs containing both vitamins B the necessary ratio. Are especially predisposed to vitamin - About - scarcely to rachitis prematurely born children; they often need purpose of vitamin D as more than 85% of calcium stocks of a fetus are formed in the III trimester of pregnancy.
For treatment vitamin - a D-scarce rachitis higher doses of vitamin D, than apply to its prophylaxis. Reception of vitamin D for 1000 ME/sug during approximately Yusug usually normalizes concentration of a calcium and Natrii phosphas in a blood; radiological signs of convalescence appear approximately in 3 weeks. However for treatment acceleration quite often register 3000 � 4000 M E / days. Such doses are especially shown in hard cases: at a lesion of bones of a thorax and difficulty of respiration.
Some diseases are followed by disturbance of an absorption of vitamin D. If such patients don't receive in addition vitamin D, the avitaminosis can develop. Drugs of vitamin D gain special preventive value at diarrhea, a steatorrhea, obstruction of cholic ways and other gastrointestinal diseases which are followed by appreciable disturbance of an absorption. In such cases parenteral administration of vitamin can be required.
Other types of a rachitis and renal osteodystrophy. These states are characterized by disturbance of synthesis of calcitriol or sensitivity of cells to it.
Gipofosfatemichesky rachitis
The H-linked gipofosfatemichesky rachitis which is followed by disturbance of exchange of a calcium and Natrii phosphas is most widespread. Concentration of calcitriol at the same time is in norm limits though for this degree of hypophosphatemia it would be necessary to expect it rising. High doses of vitamin D (usually in combination with Natrii phosphases) improve a condition of patients, but even at treatment by vitamin D concentration of calcitriol can remain is lower than expected. REH gene mutation is the cornerstone of the most common form of the H-linked gipofosfatemichesky rachitis (HYP Consortium, 1995). The protein coded by this gene represents a neutral endopeptidase. Substrate of this enzyme isn't known, but assume that it participating in Natrii phosphas transport in kidneys. The syndromes very similar to the H-linked gipofosfatemichesky rachitis are described � auto-somno-recessive gipofosfatemichesky rachitis and autosomal and dominant gipofosfatemichesky rachitis. Exact mechanisms of inheritance and pathophysiology of these options of a disease aren't known (Econsand Drezner, 1992). Vitamin - a D-dependent rachitis like I. It is an autosoma disease which cornerstone disturbance of transformation of caltsidiol into calcitriol is. For treatment prescribe physiological doses of calcitriol (Fraser et al., 1973). Vitamin - a D-dependent rachitis like II. It is autosomal disease which is characterized by hypocalcemia, osteomalacy and rachitis, and also a total alopecia. At a research of fibroblasts of skin of such patients defects of receptor are taped. These defects can be followed or disturbance of linkng of a receptor with a ligand, or binding disturbance hormone - a receptor complex with DNA. In the latter case replacements of single amino acids in that part of the DNA-binding receptor domain which forms zinc fingers are found (Pike, 1992). Even high doses of vitamin D and calcitriol don't give effect, and sick children often need administration of calcium long i.v.,
Sometimes at teenage age improvement is observed, but the reason of the last remains obscure.
Renal osteodystrophy
This state develops at HPN. It is characterized by the slowed-down transformation of a kaltsidiol into calcitriol. The delay of Natrii phosphas leads to depression of concentration of the ionized calcium in a blood and, as a result, to a secondary hyperparathyreosis. Besides, because of deficiency of calcitriol the calcium absorption in an intestine and mobilization of a calcium from bones is broken. The hypocalcemia is usually observed (though at some patients the long expressed hyperparathyreosis sometimes leads to a hypercalcemia). In a lesion of a skeleton also adjournment of aluminum in bones can play a part.
Hyperparathyreosis signs (fibrous ostitis), vitamin D deficiency (osteomalacy) or both that, and another are morphologically observed. Treatment of patients with HPN by which don't carry out dialysis is referred generally on elimination of hyperphosphatemia and rising of concentration of the ionized calcium to bloods. For this purpose prescribe a diet with the low maintenance of Natrii phosphases, fosfatsvyazyvayushchy agents and a calcium a carbonate in (Coburn and Salusky, 1989). If efficiency of analogs of vitamin D at patients who don't need dialysis yet is only checked, then at patients to whom dialysis is already carried out, it is proved. Administration of calcitriol increases concentration of a calcium in a blood, reduces the PTG level and promotes a mineralization of bones and continuation of body height at children (Berl et al., 1978; Chesney et al., 1978). At inefficiency of administration of drug i.v. introduction inside can help (Andress et al., 1989). Prescribe also Dihydrotachysterolum as I they are active without hydroxylation in kidneys. Use and caltsifediola is possible, but it helps only with high doses.
Other indications
Apply at a hypophosphatemia against the background of Fankoni's syndrome. Purpose of high doses of vitamin D (more than 10 LLC ME/sut) at an osteoporosis is deprived of sense and can be dangerous. However it is established that administration of vitamin D in doses of 400 � 800 ME/days to elderly men and women with an osteoporosis slows down processes of updating of a bone tissue, promotes conservation of its weight and reduces risk of fractures (see. "Osteoporosis"). Clinical tests testify to prospects of use of calcitriol for treatment of a psoriasis (Holick, 1993; Kragballe, 1992). As all new unusual effects of vitamin D are found, development of its analogs which are influencing a cellular differentiation, but not causing a hypercalcemia becomes more important.
Side effects
High doses of vitamin D increase risk of death from cardiovascular diseases, scientists from University of Copenhagen warn.
From the point of view of public health care, the vitamin D disadvantage is an important problem in many countries for a long time. Several researches showed that too low levels of this vitamin can be unhealthy. Nevertheless, the new research for the first time showed that too high levels of vitamin D in a blood are bound to the increased risk of death from a stroke.
Scientists considered vitamin D levels at 247574 Danes and analysed their mortality for seven years. During this time 16645 patients died. The research confirmed that there is a correlation between high death rate and too low level of vitamin D, but new opening also was the fact that too high levels of vitamin D led to death too. If the level of vitamin D is lower 50 or the 100th nmol on liter is higher, the risk of death increases, experts say. At indicators of concentration of vitamin D above the 100th nmol/litre increases risk to die of a stroke or an infarct.
In other words, the level of vitamin D shouldn't be too low, but also shouldn't be too high. According to experts, this value has to be somewhere between the 50 and 100 nmol on liter, and the 70th nmol on liter is the most preferable level.