Cart
Cart

Androgens
01 Nov 2016
Androgens (Greek ανδρεία (courage, bravery) + Greek γένος (a sort, a knee)) — the general collective name of group of the steroid hormones produced by gonads (testicles at men and ovaries at women) and a cortex of adrenals and having property in certain concentration to cause androgenesis, virilescence of an organism — development of men's secondary sexual characteristics — in both floors.
Women have androgens in concentration, characteristic of men, cause augmentation of the sizes of a clitoris and vulvar lips and rapprochement of vulvar lips (that makes them more similar to a scrotum), a partial atrophy of mammary glands, a uterus and ovaries, the termination of a menses and ovulations, sterility.
Natural androgens
- Testosterone - an inactive form
- Digidrotestosteron
- Degidroepiandrosteron (Dehydroepiandrosterone, DHEA)
- Androstenedione (Andro)
- Androstenediol
- Androsterone
Androgensin bodybuilding
In bodybuilding anabolic steroids are widely applied, however it is necessary to give preference to those medicines which have the smallest androgenic activity, they promote increase in muscle bulk, at the same time cause such side effects less as: the acne, irritability, baldness, seborrhea, a prostate hypertrophy, a masculinization, and the most important, steroids with low activity to a lesser extent cause an atrophy of testicles and after a cycle the natural level of testosterone is restored better and more stoutly. It is connected with the fact that steroids with high androgenic activity contact more androgenic receptors which settle down in a hypophysis and a hypothalamus therefore gonadotrophin level decreases.
Though recently data on androgenic activity are exposed to insinuations from laymans which spread the false information that anabolic and androgenic activity is concepts not applicable to steroid hormones.
Clinical pharmacology
Biosynthesis of androgens
Testosterone — the main androgen at men and, apparently, at women. At men his most part is synthesized in cages of Leydiga. At women testosterone is synthesized in the same way, but in a yellow body and bark of adrenal glands. Predecessors of testosterone androstenedione and dehydroepiandrosterine have weak androgenic activity.
Secretion and transfer by blood
Practically at any age at men more testosterone, than at women is formed, and it explains almost all distinctions between floors. In the I trimester of pregnancy testicles of a fruit begin to emit testosterone (possibly, under the influence of secretable HG placenta) which plays the main role in formation of male genitals. By the beginning of the II trimester its serumal concentration becomes almost same, as in the middle of the pubertal period — about 250 mg % (fig. 59.2) (Dawood and Saxena, 1977; Forest, 1975). By the end of the II trimester she falls, but to childbirth reaches about 250 íă % again (Forest and Cathiard, 1975; Forest, 1975; Dawood and Saxena, 1977), perhaps, due to stimulation of cages of Leydiga L G, formed in a fruit hypophysis. In the first days of life concentration of testosterone decreases again, then by 2 — 3 months rises to 250 ng % and further falls lower than 50 ng %, remaining at such level prior to the beginning of the pubertal period (Forest, 1975), From 12 — 17 years concentration of testosterone at boys increases much stronger, than at girls, by the end of teenage age reaching 500 — 700 and 30 — 50 ng % respectively. At men high concentration of testosterone provides puberty and further development of secondary sexual characteristics. With age she gradually decreases, bringing, perhaps, various manifestations of aging.
LG, secretable gonadotrophic cells of a hypophysis (hl. 56) — the main stimulator of secretion of testosterone. Perhaps, L G action amplifies in the presence of FSG — the second hormone of these cells. In turn, stimulates secretion of LG gonadropin, formed in a hypothalamus, and brakes testosterone which directly affects gonadotropin cells. Secretion of LG happens pulsewise, the interval between peaks of secretion makes about 2 h, and amplitude of peaks is higher in the morning. Such nature of secretion of LG, apparently, is defined by impulse secretion of gonadoliberin in a hypothalamus. In case of a hypothalamic gipogonadizm impulse introduction of gonadoliberin normalizes L G secretion and testosterone whereas the long infusion of gonadoliberin doesn't help (Crowley et al., 1985).
Testosterone secretion also happens pulsewise and generally in the afternoon. Its concentration is maximum at 8:00 and is minimum at 20:00. With age morning concentration of testosterone decreases (Bremner et al., 1983).
Causes production of testosterone in the yellow body which is formed on the place of a follicle after an ovulation in L G women. However as normal main inhibitors of secretion of LG at women serve the estradiol and progesterone, but not testosterone. In blood about 2% of testosterone are in a free form, 40% strongly are kept by the globulin connecting sex hormones, and other testosterone is unsteadily connected with albumine.
Metabolism
Testosterone has various effect on many fabrics. One of the reasons of such variety — transformation of testosterone into two other steroid hormones, dihydrotestosteron and an estradiol (fig. 59.3). Testosterone causes one effects itself, others are rendered by dihydrotestosteron, the third — an estradiol.
Irreversible restoration of testosterone in dihydrotestosteron is catalyzed by 5a-reductase. Both hormones activate the same androgenovy receptors, but dihydrotestosteron has bigger affinity to receptors (Wilbert et al., 1983) and stronger influences an expression of genes (Deslypere et al., 1992). Turning into dihydrotestosteron in the fabrics containing a 5a-redukgaza, testosterone can make on them additional impact. Two types of 5a-reductase are described: type 1 (mainly in a liver and extregenital sites of skin) and type 11 (in uric ways and genitals at men, and also in skin of genitalia at men and women). Effect of dihydrotestosterone on these fabrics is described below. Do not forget take Cortexin for better results.
Testosterone is inactivated in a liver with formation of an androsteron and etiokholanolon. Dihydrotestosteron turns in androsteron, androstandion and androstandiol.
Physiological effects and mechanisms of action
Effects of testosterone depend on what receptors it affects, and also from fabric and from age of the person. Testosterone renders as androgenic action, contacting androgen receptors directly or after transformation into dihydrotestosteron, and estrogenic, by transformation into estradiol and activation the estrogen of receptors.
Action on androgen receptors. Testosterone and dihydrotestosteron stimulate the same androgen receptors which concern to the group of intracellular receptors including also receptors of steroid hormones, thyroid hormones, calcitriol, retinoid and a number of receptors with unknown ligands. Testosterone and dihydrotestosteron interact with the receptor domain of a receptor that hormone allows - receptorly to a complex by means of the DNA-connecting domain to contact certain genes. The hormone-receptor complex works as a transcription factor, strengthening an expression of these genes (Brinkmann and Trapman, 2000).
Only in recent years there were data on the reasons of a variety of effects of androgens in various fabrics. One of them — higher affinity of dihydrotestosterone to androgenovy receptors in comparison with testosterone (Deslypere et al., 1992; Wilbert et al., 1983). Recently also other mechanism connected with transcription factors (coaktivators and korepressor), specific to various fabrics has been described.
Value of androgen receptor is accurately revealed by consequences of mutations of the gene coding it. As one would expect, the mutations changing primary structure of protein (there is enough replacement of one amino acid in DNA-connecting or receptor domains), cause resistance to testosterone already in the pre-natal period (McPhaul and Griffin, 1999). It leads to violation of a sexual differentiation and a delay of sexual development.
The mutation of other type causes the H-linked bulbospinal amyotrophy (Kennedy's syndrome). At such patients the number of repetitions of TsAG coding a glutamine because of what the polyglutamic site on the N-end of a receptor is extended (Laspada et al is increased., 1991). It reduces sensitivity of a receptor to androgens only a little, but leads to the progressing atrophy of motor-neurons (the mechanism of the last isn't known).
At last, mutations explain development of resistance to anti-androgenic therapy at the spreading prostate cancer. In the beginning the tumor happens hormonal and dependent, at least partly what anti-androgenic therapy is based on. Often in the beginning the tumor will respond to treatment and her sizes decrease, but then stability is developed. At such patients various mutations of a gene of androgen receptor because of what the receptor can be activated by other ligands or in general for lack of a ligand (Visakorpi et al are described., 1995).
Action on estrogen receptors
Transformation into estradiol under the influence of aromatase explains influence of testosterone on bones, and it is possible, and on some other fabrics. In those exceptional cases when in an organism of the man are absent an aromatase (Carani etal., 1997; Morishmaetal., 1995) or estrogenovy receptors (Smith et al., 1994), epiphyseal zones of growth are not closed and tubular bones grow beyond all bounds long; besides, osteoporosis develops. The estradiol eliminates all these violations at insufficiency of an aromatase (Bilezikian et al., 1998), but not at defect the estrogen receptors. There are data that transformation of testosterone into estradiol defines sexual behavior of males of rats, but the similar effect at people is not revealed.
Androgens during the different periods of life
Pre-natal period. Approximately on the 8th week of pregnancy under the influence of HG testicles of a fruit begin to emit testosterone. Local increase in concentration of testosterone in wolffian ducts in internal male genitals causes a differentiation: small egg appendages, seminal ducts and seed bubbles. In laying of genitalia testosterone turns into dihydrotestosteron under the influence of which the penis and a scrotum, and also a prostate gland develop (George and Wilson, 1992). Strengthening of secretion of testosterone by the end of pre-natal development causes growth of a penis.
Newborns. Value of the increased secretion of Testosteron-Depotum in the first months of life isn't known.
Pubertal period. At men this period begins approximately in 12 years with rising of secretion of a gonadoliberin in a hypothalamus. It strengthens development by gonadotrophic cells of FSG and LG which promote body height of testicles. The augmentation of testicles is the first sign of puberty. The strengthened synthesis of Testosteron-Depotum along with action of FSG on Sertoli's cells stimulates development of a wavy seed canaliculus in which spermatozoons are formed. Rising of concentration of Testosteron-Depotum in a blood at the same time influences many tissues, but changes in most of them happen gradually, within several years. Length and thickness of a penis are enlarged, there are scrotum cords, the prostate gland begins to excrete the secret which is a part of a semen. Production of dermal fat increases, the skin becomes more rasping and fat that promotes development of acnes. There are hair in axillary hollows, on a pubis, then on anticnemions and at last on other parts of a body and on a face. Development of a pilosis can take about 10 years, its end speaks about the end of the pubertal period. The weight and force of muscles, especially muscles of a shoulder girdle increase, the hypodermic fat becomes thinner. Tubular bones are quicker extended that leads to the general acceleration of body height, however epiphyseal zones of body height are gradually closed because of what body height is slowed down and as a result stops. Bones are at the same time thickened. As a result of rising of mass of muscles and a bone tissue weight is considerably enlarged. The erythrogenesis amplifies, and concentration of a hemoglobin at men becomes higher, than at boys and women. Cartilages of a larynx are thickened and the voice goes down. Sexual desire develops.
Rising of concentration of Testosteron-Depotum in the pubertal period affects also nervous activity: men are guided in space usually best of all, and their behavior in a number of the relations differs from behavior of women, in particular men are more aggressive.
Mature age. At young and middle age both serumal concentration of testosterone, and characteristic features of the adult man almost don't change. However the androgenetichesky alopetion beginning with emergence of high temples and a hair loss on a darkness gradually develops.
Much more changes in a prostate gland have bigger medical value. First, at all men prostate gland adenoma in a varying degree develops. Sometimes it leads to sdavleniye of an urethra and violation of outflow of urine. Emergence of adenoma is connected with transformation of testosterone into di hydrotestosteron in cells of a prostate gland under the influence of 5a-reductase of type II (Wilson, 1980). One of modern approaches to treatment of adenoma of a prostate gland is based on inhibition of this enzyme (McConnell et al. 1998), as it is described below.
Secondly, the prostate cancer can develop. Though there are no direct proofs of an etiologichesky role of testosterone, the tumor is hormonal and dependent, at least partially and during some time. In this regard at a meta-staziruyushem prostate cancer seek to reduce concentration of testosterone (Huggins and Hodges, 1941; Iversen et al., 1990).
Advanced age. With age serumal concentration of testosterone gradually falls, at the same time concentration of the globulin connecting sex hormones grows. By 80 years the general concentration of testosterone makes about 85%, and concentration of free testosterone — only about 40% of the corresponding concentration in 20 years (Purifoy et al., 1981; Deslypereand Vermeulen, 1984). Such age changes as reduction of working capacity, sexual desire, muscle bulk (Forbes, 1976) and forces can be connected with falling of concentration of testosterone (Murray et al., 1980), and also density of a bone tissue (Riggs etal., 1982). Point out similar changes at a gipogonadizm at young men this dependence (see below).
Deficiency of androgens
Consequences of deficiency of androgens depend on degree of deficiency and age at which it arose. Pre-natal period. In the I trimester of pregnancy deficiency of testosterone at a fruit conducts to an incomplete sexual differentiation. Only changes in testicles can be the cause of deficiency of testosterone (for example, insufficiency of a 17a-hydroxylase): the lack of LG at diseases of a hypophysis or hypothalamus at this stage of development does not result in deficiency of testosterone as in the beginning testosterone secretion by cages of Leydiga is regulated by HG.
For lack of testosterone external female genitals are formed; in less hard cases there is an incomplete virilization and ambiguous genitalia develop, their structure depends on testosterone level. Also the differentiation the volfovykh of channels is broken to semyavynosyashchy canals and seed bubbles, at the same time sekretiruyemy testicles a regression factor the myullerovykh of channels does not allow them to develop in female genitals. Similar changes happen also at normal secretion of testosterone if its activity is reduced owing to defect the androgenovykh of receptors or insufficiency of 5a-reductase. Different defects the androgenovykh of receptors meet. In the most hard cases the receptor is completely inactive, and testicular feminization with development of external female genitals is observed. In medium-weight cases there is their incomplete virilization; in mild cases only the spermatogenesis at adults is broken (McPhaul and Griffin, 1999). Insufficiency of 5a-reductase is followed by an incomplete virilization of genitalia at normal development internal as the last depends on testosterone (Wilson et al., 1993).
Deficiency of Testosteron-Depotum in the III trimester of pregnancy because of illnesses of testicles or deficiency of LG at a fetus leads to two disturbances. First, there is no normal body height of a penis and there are microsinging. It is often observed at boys with L G deficiency caused by disturbance of synthesis of a gonadoliberin. Secondly, testicles don't fall to a scrotum, that is there is a cryptorchism; this state is also quite often observed at L G deficiency.
Pubertal period. If at the boy in the fetal period Testosteron-Depotum is synthesized normally, and its deficiency arises before the pubertal period, then the delay of sexual development is observed. Depending on degree of deficiency the changes of external genitals described above, piloses, the muscle bulk, a voice and behavior are to some extent slowed down. Besides, at normal secretion of STG against the background of Testosteron-Depotum disadvantage of puberty age closing of epiphyseal zones of body height is late that leads to excess elongation of tubular bones and disproportionate body height of arms and legs concerning a trunk because of what the body build becomes eunuchoid. At last, the glandular tissue of mammary glands expands and there is a gynecomastia.
Mature age. If deficiency of Testosteron-Depotum arises after completion of sexual development, there is involution of secondary sexual characteristics, and expression of this process depends on degree and duration of deficiency. In hard cases already in 1 — 2 week depression of sexual desire and working capacity is observed, other symptoms develop more slowly. Depression of muscle bulk and force on average happens in several months, but for emergence of noticeable changes in certain patients years are required.
Within several months there is an essential depression of a hematocrit and concentration of a hemoglobin. The two-photon x-ray absorbtsiometriya is capable to find depression of density of a bone tissue in 2 years though the risk of fractures increases only in many years. Decrease of a pilosis on men's type also happens gradually, for many years. Deficiency of androgens at women reduces a pubic and/1 axillary pilosis, but it becomes noticeable only in several years. At women androgens, perhaps, perform also other important functions lost in their absence (especially at the combined deficiency of ovarian and adrenal androgens against the background of an apituitarism). Testosteron-Depotum drugs which can maintain physiological concentration of this hormone at women are now developed. Use of these drugs will allow to learn how replacement therapy by Testosteron-Depotum at deficiency of androgens at women is capable to raise sexual desire, weight and force of muscles, density of a bone tissue and working capacity.
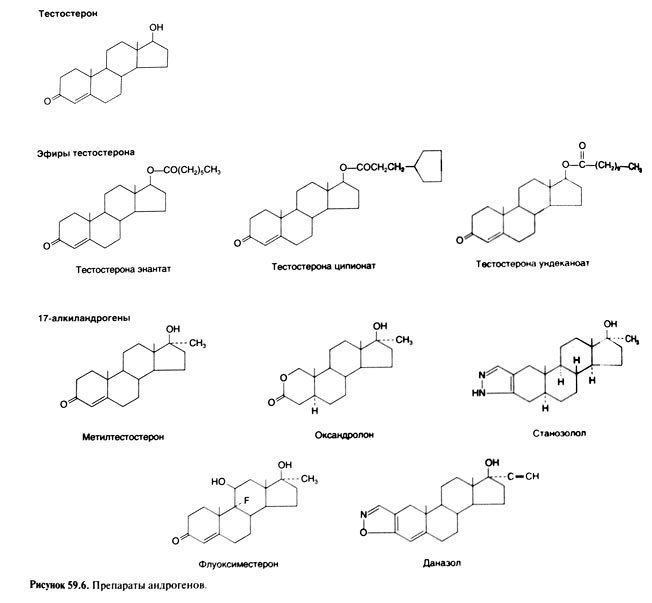
Medicines of androgens
At intake testosterone is inefficient: he is well soaked up, but quickly inactivated in a liver. Therefore for maintenance of normal serumal concentration of testosterone medicine should be accepted too often and in too high doses. Respectively, the majority of medicines of androgens have the structure interfering their fast destruction in a liver. Besides, search of the medicines possessing more selective action is conducted.
Medicines of androgens for skin application
Other opportunity to avoid an inactivation of the entered testosterone is use of a plaster from which not changed hormone slowly is soaked up through skin. Daily gluing of a plaster allows to reduce fluctuations of concentration of testosterone in comparison with introduction of his air in oil. The first such plasters were pasted on scrotum skin (Findlay et al., 1989). Here skin so thin that testosterone is soaked up in enough and without addition of the substances facilitating absorption. Then the plasters containing such substances have been developed thanks to what these plasters could be pasted on other sites of skin (Yu et al., 1997; Dobs et al., 1999). Testosterone medicine in the form of aqueous-alcoholic gel is recently created (Wang et al., 2000). All these medicines put 1 time a day that provides normal concentration of testosterone at the majority sick gipogenitalism.
Search of selective androgens
Alkylandrogens
Half a century works on synthesis of analogs of testosterone with prevalence of anabolic activity over androgenic were conducted back. It seemed, a number of substances had such properties as at rats they exerted a greater influence on the muscle lifting back pass than on forward department of a prostate gland (Hershberger and Meyer, 1953). These substances were called anabolic steroids, most of them was 17 alkylandrogens. However any of them didn't show desirable selectivity at people. Nevertheless anabolic steroids are widely applied by athletes as dope (see below). Feature of other alkylandrogen, 7a-methyl-19-nortestosterona — resistance to effect of 5a-reductase (Kumar et al., 1992). The selective modulators androgenovykh of receptors. Creation of the selective modulators estrogen receptors (tamoxifen, raloksifen) activating estrogenovy receptors in one fabrics and blocking in others stimulated development of similar modulators the androgen receptors
However, selectivity of raloksifen, apparently, is connected with big affinity to one isoform the estrogen receptors prevailing in bones and in a myocardium and smaller affinity to other form characteristic of a mammary gland and endometrium. As only one form androgen receptors is found, selective action on them has to be based on fabric specificity of coactivators and corepressor — the proteins regulating influence of intracellular receptors on a transcription of genes targets (Moilanen et al., 1999). The group of quinolines with selective androgenic activity is received (Zhi et al., 1999).
Application of androgens
The obvious indication to purpose of androgens — deficit of testosterone (gipogonadizm) at men. Androgens apply also in other cases; possibly, new indications to their appointment in the future will appear.
Men hypogenitalism. In case of deficit of testosterone appoint any of testosterone medicines described above for skin application or testosterone air. At teenagers and elderly it is necessary to watch efficiency and safety of treatment especially carefully.
efficiency evaluation
The treatment purpose — maintenance of serumal concentration of testosterone as is possible closer to normal therefore measurement of this concentration serves as the main evaluation method of efficiency of treatment. Time of measurement depends on medicine: if testosterone medicines for skin application are used, concentration can be determined in any day and at any time. At the same time it is necessary to consider that concentration reaches a maximum in 2 — 4 h after gluing of a plaster for scrotum skin (Findlay et al., 1987) or a plaster Testoderm for the ekstragenitalnykh of sites of skin (Yu etal., 1997) and in 6 — 9 h when using a plaster Androderm for the ekstragenitalnykh of sites of skin (Dobs et al., 1999), and the minimum concentration before gluing of the following plaster makes 60 — 70% maximum (Findlay et al., 1987). When using gel serumal concentration of testosterone within a day changes a little, but stationary concentration of medicine is sometimes established only in a month after an initiation of treatment. When using testosterone of an enantat or tsipionat, entered each 2 weeks, concentration of testosterone is measured in the middle of this interval. The measured concentration of testosterone shan't differ from normal, otherwise the mode of introduction is changed. If deficit of testosterone is caused by defeat of testicles (in this case concentration of LG is increased), normalization of concentration of LG within 2 months after the beginning of replacement therapy testifies to efficiency of treatment (Snyder and Lawrence, 1980; Findlay etal., 1989).
Normalization of serumal concentration of testosterone at men with hypogonadism leads to completion of development of secondary sexual characteristics and their maintenance. Within several weeks at such men sexual desire and working capacity have to raise (Davidson et al., 1979). In several months the muscle bulk and force increase and the mass of fatty tissue decreases (Katsnelson et al., 1996). Density of a bone tissue reaches a maximum within 2 years (Snyder et al., 2000).
Side effects of Testosteron
Testosteron-Depotum drugs for cutaneous use and Aethers of Testosteron don't possess any action other than action of endogenic Testosteron (if the therapeutic dose isn't exceeded). However when performing replacement therapy there can be undesirable effects. Some of them appear soon after an initiation of treatment, others — usually only in several years. Rising of concentration of Testosteron from the level of prepubertatny or the middle of the pubertal period to the level characteristic of the adult man, can conduct to such phenomena inherent to the pubertal period as an acne, a gynecomastia and aggressive sexual behavior. Physiological quantities of Testosteron don't influence a blood lipid profile. Replacement therapy sometimes has undesirable effect at associated diseases. So, stimulation of erythrogenesis leads to normalization of hematocrit at the man healthy for the rest, however at predilection to hyperglobulia (for example, against the background of HOZL) the hematocrit can exceed norm. In a similar way the small delay of sodium and water won't affect the healthy person, but will aggravate a heart failure. At Testosteron overdosage the hyperglobulia and, occasionally, a water delay with edemas develop also for lack of predisposition to these states. When normal concentration of Testosteron is maintained for many years (due to its endogenic secretion or replacement therapy), 40 years are aged more senior the risk of such hormonal and dependent states as adenoma and a prostate cancer increases.
Testosteron derivatives 17 alkylandrogens possess a side effect on a liver, sometimes causing a cholestasia and, occasionally, ďĺëčîç a liver (formation of the lacunas filled with a blood). Separate cases of pechenochnokletochny cancer are described, but the etiological role of these drugs is doubtful. Besides, 17 alkylandrogens, especially in high doses, reduce the LPVP level.
Hypogonadism in the pubertal period. If the hypogonadism is observed at boys, then in the pubertal period prescribe it Testosteron drugs, proceeding from the principles stated above. It is important to remember that Testosteron accelerates closing of epiphyseal zones of body height therefore at first it causes rapid growth, but then body height finally stops. Respectively, it is necessary to consider body height of the boy and the STG level at it. With a low growth and deficiency of STG at first prescribe somatropin, and already then treat hypogonadism.
Aging at men. According to preliminary data, replacement therapy by Testosteron at men with age depression of concentration of this hormone increases density of a bone tissue and body weight and reduces the mass of fatty tissue (Snyderet ah, 1999a, b). However it isn't clear whether body height of adenoma of a prostate causes such treatment, and whether the risk of the prostate cancer which is shown clinically is enlarged. Hypogonadism at women. It isn't proved yet that purpose of Testosteron to women with the lowered serumal concentration of Testosteron promotes body height of sexual desire, working capacity, muscle bulk and force, and also density of a bone tissue.
Dope. For achievement of the best results some athletes resort to dope, including use androgens. Usually these drugs accept secretly therefore their action is studied worse, than effect of the drugs prescribed at treatment of hypogonadism. Drugs. Athletes used almost all androgens applied in medicine and veterinary science as dope. It began more than 20 years ago, and initially preference was given to anabolic steroids — 17 alkylandrogens and other substances which were allegedly possessing mainly anabolic action in comparison with Testosteron. As such bonds can be easily taped by the controlling larger distribution was gained by HG and Aethers of Testosteron increasing serumal concentration of Testosteron-Depotum. In recent years use of precursors of Testosteron (androstendion and degidroepiandrosteron) which aren't entering lists of banned drugs was enlarged. Efficiency. The majority of the tests devoted to influence of Testosteron on an animal force were uncontrollable. In one double blind test 43 persons (all men) were divided into 4 groups: in the first two groups examinees carried out power exercises against the background of introduction of Testosteroni oenanthas in a dose of 600 mg once a week (more than 6 times higher, than at replacement therapy) or placebo, in the third and fourth groups examinees received the same drugs for lack of exercises. Testosteron enlarged body weight and an animal force, and exercises gave additional effect (Bhasin et al., 1997).
In other double blind test androstendion (on 100 mg 3 times a day during 8 weeks) didn't lead to increase in muscular force in comparison with placebo. However, it isn't surprising as average concentration of testosterone also didn't increase (King et al., 1999).
Side effects of androgens
At reception of therapeutic doses of any androgen some side effects arise always; emergence of other effects depends on medicine or additional conditions. All androgens in high doses suppress secretion of LG and FSG, oppressing functions of testicles: production of endogenous testosterone and spermatozoa falls that ability to fertilization. Reception of androgens for many years can lead to reduction of testicles. Function of testicles is usually restored in several months after medicine cancellation, but sometimes more time for this purpose is required. High doses of all androgens cause erytrocytosis (Drinka et al., 1995);
Androgens capable to turn into estrogen (first of all testosterone), in high doses cause ginecomastia. Medicines with the modified ring and, not exposed to aromatization, for example dihydrotestosteron, are deprived of this action.
Hepatotoxic action is peculiar only to 17 alkylandrogens (see above). Besides, in high doses they are more often than other androgens break lipidic exchange, reducing the LPVP level and increasing the LPNP level. There are unconfirmed messages on such side effects as mental disorders and the sudden death from IBS which is presumably connected with change of a lipidic profile and increase in coagulability of blood.
Some side effects of androgens are especially noticeable at women and children — character of pilosis peculiar to men, high temples and eels. At boys the penis increases, women have a clitoris. Boys and girls stop growing because of premature closing the epiphyseal zones of growth. Contraception at men. The contraceptives for men containing androgens are developed (including in combination with other medicines). Their action is based on suppression of secretion of LG in a hypophysis and the subsequent reduction of synthesis of endogenous testosterone. Normal concentration of testosterone in testicles approximately by 100 times exceeds that in blood. High concentration of testosterone is necessary for a spermatogenesis, her decrease sharply slows down this process. However, in the first attempts of use of testosterone suppression of a spermatogenesis required twice a big dose of testosterone enantat, than for replacement therapy, and all the same it wasn't possible to suppress completely a spermatogenesis at all men (WHO Task Force for the Regulation of Male Fertility, 1996). In other early tests the antagonists of gonadoliberin suppressing secretion of LG in combination with replacement therapy by testosterone applied (Pavlou et al., 1991). However such combination isn't suitable for broad application as the available antagonists of gonadoliberin it is necessary to enter in the form of the daily injections causing emission of a histamine. The combination of progestagen to physiological doses of testosterone for suppression of secretion of L G and a spermatogenesis at preservation of normal serumal concentration of testosterone is more perspective (Bebb et al., 1996). Now pass testosterone test undecanoat for injections, providing rather stable serumal concentration of testosterone within a month (Zhang et al., 1999), and 7a-methyl-19-nortestosteron, the synthetic androgen which isn't restored by 5a-reductase and therefore not acting on a prostate gland (Cummings et al., 1998).
Exhaustion. Anabolic activity of testosterone was tried to be used for treatment of an atrophy of muscles and exhaustion, but in most cases this method was inefficient. The exception makes treatment of the atrophy of muscles at AIDS which is followed by gipogonadism. At patients with AIDS of men with an atrophy of muscles and the lowered serumal concentration of testosterone such treatment increases the muscle bulk and force (Bhasin et al., 2000).
Quincke's edema. Continuous treatment by androgens prevents Quincke's edema attacks. Illness is bound to heriditary failure of an inhibitor of C1 esterase or development of antibodies to it (Cicardi et al., 1998). 17 alkylandrogens (stanosolol and danasol) stimulate synthesis of an inhibitor of C1 esterase in a liver. Unfortunately, they cause virilescence in women. Because of virilescence and premature closing of epiphyseal zones of body height androgens don't use for prophylaxis of Quincke's edema at children, but sometimes prescribe them at attacks. Illnesses of a blood. Before emergence of erythropoetin androgens applied to stimulation of an erythrogenesis at anemias of various etiology. Androgens (in particular, danasol) still sometimes prescribe at the hemolitic anemia and an idiopathic Werlhof's disease steady against standard treatment.