Cart
Cart

Parkinson's disease-risk factors and approaches to therapy
20 Jul 2017
Neurologist Dr. Doping speaks about parkinsonism syndrome, dopamine deficiency and development of methods of neuroprotection.
Parkinson's disease is a chronic progressive neurodegenerative disease of the brain. Descriptions of the manifestations of the disease were discovered even in the works of ancient Indian doctors - Ayurveda. But the discoverer of the disease recognized English physician James Parkinson, who published in 1817 the essay "Essay on the trembling paralysis," which described several cases and noted a number of characteristic symptoms of the disease. A more complete description of the clinical picture of the disease was made in the 1860s by the French neurologist Jean Martine Charcot, who suggested that the disease should be named after James Parkinson.
Symptoms of Parkinson's Disease
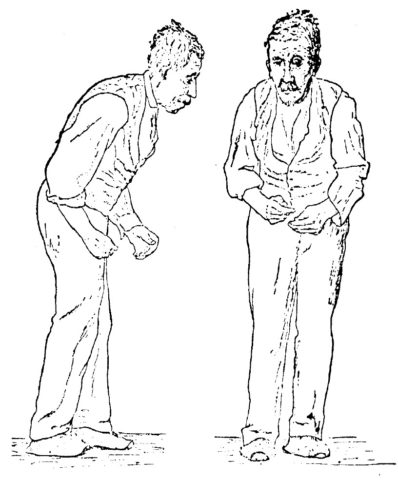
Parkinsonism syndrome is the key in the clinical picture of the disease. It is manifested by slowing down the tempo and decreasing the amplitude of movements (bradykinesia) in combination with increased muscle tone and / or tremor (tremor) of the hands, legs, chin. The key violation is bradykinesia, and tremor in a quarter of cases of the disease is completely absent.
Bradykinesia can be manifested by a decrease in the loudness of the voice and a violation of articulation, a depletion of facial expressions, a decrease in the size of letters in writing, the restriction of small finger movements, parkinsonic gait (decrease in height and step length), slowing and difficulty getting up from the chair, turning in bed. Bradykinesia, changes in muscle tone and posture are often manifested by pain or discomfort in the arm (shoulder joint), back. With Parkinson's syndrome in later stages of the disease, instability is combined with possible falls, disturbances in the beginning of walking, episodes of involuntary stops ("congestion") during walking.
Isolate the form, where the predominant tremor (mainly the trembling form), akinetic-rigid (without tremor) and mixed. It is noted that akinetic-rigid form often proceeds more severely - with a relatively rapid increase in violations of walking, instability, disorders in the intellectual sphere. Parkinson's disease is marked by a significant variability in the course of the disease with different degrees of motor and non-motor manifestations of the disease.
Causes of Parkinson's Disease
There is as yet no definitive answer to the question of the root cause of the onset of Parkinson's disease. Researchers continue to study the causes of premature aging and death of nerve cells. It is believed that the development of the disease is caused by the interaction of hereditary predisposition, external neurotoxic factors and aging processes. Some inherited genes increase the vulnerability of nerve cells to the effects of damaging environmental factors.
To external harmful factors include salts of certain metals, organic solvents, pesticides and herbicides. The list of substances potentially dangerous for nerve cells continues to expand. As a result of this interaction, a cascade of neuropathological reactions is triggered. Thus, a widespread neurodegenerative process is formed, which affects various parts of the brain and the peripheral autonomic nervous system as the disease progresses.
Lewy bodies
An important milestone in the study of Parkinson's disease is associated with the discovery of the morphological substrate of the disease. In 1919, the Soviet neurologist Konstantin Tretyakov linked the development of Parkinson's symptoms with the loss of special brain cells - the pigment neurons of the black substance of the trunk, as well as the deposition of pathological inclusions in these cells. Neurological inclusions Tretyakov suggested calling Lewy bodies in honor of the German morphologist Friedrich Levy, who previously described similar changes in parkinsonism in other parts of the brainstem. This discovery is fundamental in understanding the pathological changes underlying the motor symptoms of the disease.
Dopamine deficiency
The occurrence of motor manifestations of Parkinson's disease is associated with the premature death of brain nerve cells that produce dopamine. In 1958, Swedish pharmacologist Arvid Karlsson, carrying out experiments on animals, proved the significant role of dopamine in the brain. Half a century later, he received the Nobel Prize for this discovery. A significant decrease in the content of dopamine in the median structures of the brain (basal ganglia) in patients who died from Parkinson's disease was shown in 1961 by an Austrian scientist Oleg Gornyevich.

Dopamine is a neurochemical substance necessary for the transmission of nerve impulses in brain cells that provide the ability to move. Lack of dopamine, in turn, is the main cause of motor disorders in patients. However, the deficiency in dopamine production is manifested not only by impairments in the motor sphere. Dopamine is involved in the regulation of emotions, motivational components of behavior, cognitive processes. Therefore, disorders of the emotional, intellectual sphere, behavior are very characteristic for Parkinson's disease.
Morphology in Parkinson's Disease
In recent decades, the notion of morphology in Parkinson's disease has been significantly expanded, evidence of the prevalence of the pathological process in this disease has been obtained. In addition to the deficiency of dopamine, "suffering" and other neurochemical brain systems have been proven. So, with the degeneration of the brain stem nuclei, which produce other neurotransmitters (serotonin, noradrenaline, acetylcholine), the development of depression, anxiety, apathy, sleep disorders and increased daytime sleepiness, and the violation of intellectual functions are associated. These symptoms in different combinations at different stages of the disease occur in 30-80% of patients and can outstrip the motor classic symptoms of the disease by 5-10 years, forming the so-called pre-motor stage of the disease. Parkinson's disease can begin with nedofaminergic brain structures.
Diagnostic Methods
The diagnosis of "Parkinson's disease" is established on the basis of an analysis of the medical history - anamnesis and clinical examination data. Neuroimaging of the brain (magnetic resonance imaging) is used to exclude other diseases (brain tumors, hydrocephalus, discirculatory encephalopathy) and is prescribed mainly when atypical, uncommon for Parkinson's disease, anamnestic data or clinical symptoms.
Modern methods of neuroimaging (single photon emission computed tomography, positron emission tomography) with the introduction of various radiopharmaceuticals allow us to evaluate the functional state of the endings of neurons that produce dopamine in the brain, according to the degree of absorption of radioactive analogs of dopamine. These methods are used mainly in scientific research, can be used in diagnostically complex cases. But the high cost of modern methods of neuroimaging does not allow them to be widely used in clinical practice.
To confirm the diagnosis of "Parkinson's disease", especially with initial manifestations, ultrasound can be performed - transcranial sonography. In this case, a marker of Parkinson's disease is an increase in the intensity of the signal (hyperechogenicity) from the black substance (sensitivity and specificity of the method is 90%). Unlike the functional methods of neuroimaging, transcranial sonography is characterized by safety and simplicity: intravenous radiopharmaceuticals are not administered. It is available from an economic point of view.
Therapy of Parkinson's Disease
The basic approach to the therapy of Parkinson's disease is symptomatic, that is, the effect on the symptoms of the disease in order to reduce their severity. A new era in the treatment of patients with Parkinson's disease began in the 1960s, when levodopa was started - it is a metabolic precursor of dopamine. Preparations containing levodopa are still the most effective means for treating Parkinson's disease. Other means are used that functionally replace the lack of dopamine: dopamine receptor agonists, amantadines, drugs that reduce the destruction (catabolism) of dopamine and levodopa.
Modern research of parkinsonism
Modern studies of Parkinson's disease cover a wide variety of aspects. One of the actively developed areas of study of Parkinson's disease is the refinement of molecular mechanisms of pathogenesis of the disease, the isolation of biochemical, clinical markers of early stages of the development of the disease. Understanding these aspects is promising in the development and implementation of effective methods of neuroprotection - approaches aimed at slowing neurodegeneration. Genetic, morphofunctional, clinical factors that allow to predict the features of the course of the disease are studied. The etiological features of the pathophysiology of non-motorized disorders of the disease, the degree of their influence on the quality of life of patients, approaches to their prevention and treatment are specified.
For symptomatic therapy, more advanced dosage forms are being developed that ensure long-term, physiological activation of the dopaminergic receptors of the basal ganglia. The prerequisites for this task are the pharmacokinetics of levodopa with a short half-life of the drug from the blood plasma, slowing down the motility of the gastrointestinal tract in patients with Parkinson's disease with impaired absorption of the drug in the late stages of the disease.